- A: Certainly. In the U.S., payers are organizations—health plans, insurance companies, government programs like Medicare/Medicaid—that finance or reimburse the cost of healthcare services. They sit at the center of healthcare financing: collecting premiums, managing risk pools, contracting with providers, adjudicating claims, and ensuring regulatory compliance. PBMs are also part of Payers world. Their influence is enormous—they shape how care is delivered, priced, and accessed.
A: Payers operate through interconnected workflows:
- - Enrollment & Eligibility – onboarding members, verifying coverage.
- - Claims Processing – receiving, adjudicating, and paying claims.
- - Provider Lifecycle Management (PLM) – credentialing, contracting, monitoring providers.
- - Appeals & Grievances (A&G) – managing member/provider complaints.
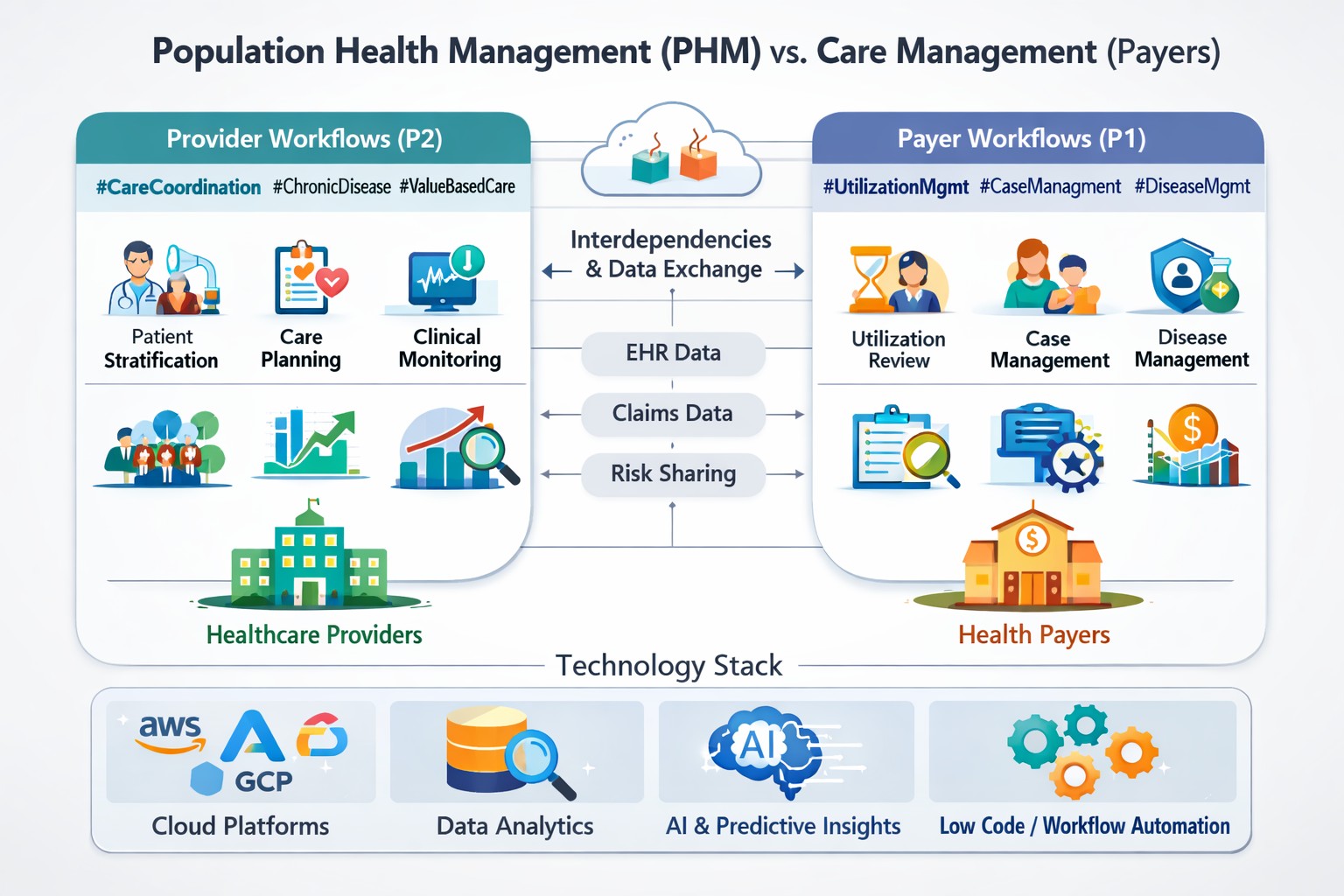
- - Utilization & Care Management (UM/CM/DM) – authorizations, case management, chronic care programs.
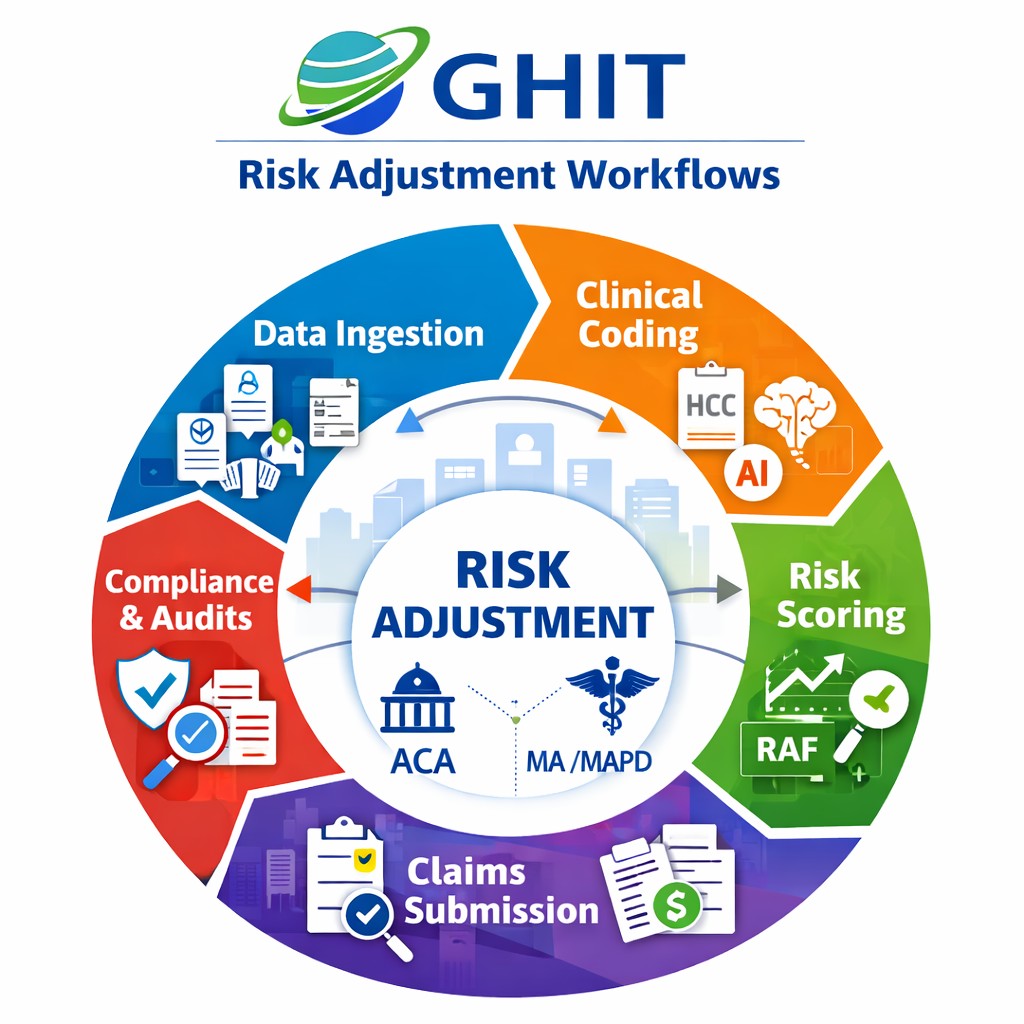
- - Risk Adjustment & Compliance – coding accuracy, regulatory reporting, audits.
- - Finance & Pricing – premium calculation, network pricing, payment integrity.
- - Member Engagement – communication, wellness programs, care gap closure.
A: Five stand out:
- Rising healthcare costs and reimbursement pressure.
- Regulatory compliance with CMS, ACA, MACRA, and state mandates.
- Member engagement & retention in an era of consumerism.
- Operational inefficiency in claims, prior auth, and appeals.
- Data silos across EHR, claims, pharmacy, CRM, and external sources.
A: Payers depend on providers for timely, accurate claims and clinical data. Providers rely on payers for reimbursement. Misaligned incentives cause friction—delayed claims, denials, and disputes. Both sides share challenges like data fragmentation, care coordination, and addressing social determinants of health. Modern interoperability standards like FHIR are helping bridge these gaps.
A: Unclosed care gaps—missed preventive screenings, medication non-adherence—lead to poor outcomes and higher downstream costs. For payers, this affects HEDIS measures and Star Ratings, which directly impact quality bonus payments. AI-powered engagement and nudging strategies can measurably increase gap closure and revenue.
A: The stack includes:
- Core Admin Systems (CAS) – Facets (Cognizant), QNXT (TriZetto), HealthEdge.
- Pricing & Payment Integrity – NetworX Pricer, ClaimsXten, Cotiviti.
- Care Management – ZeOmega, GuidingCare, CaseWorks.
- CRM & Engagement – Salesforce Health Cloud, Microsoft Dynamics.
- Workflow & Document Management – ECM/BPM/CCM from NewgenONE, Pega.
- Analytics & Risk Adjustment – SAS, Optum, bespoke AI models.
- Ancillary Apps – Provider directories, member portals, call center solutions.
A: Absolutely. Most payers operate with 10–15+ disparate systems. Without proper integration, claims get delayed, care managers lack full – 360-degree member views, and executives make decisions on partial data. Member 360—a unified longitudinal profile—is a critical integration goal, often enabled through AI-first data platforms and FHIR APIs.
A: AI reduces manual effort and accelerates decision-making. For example:
- Claims anomaly detection to recover revenue leakage.
- Prior authorization automation using NLP and GenAI.
- Risk adjustment models that predict coding gaps.
- Chatbots and GenAI agents for member inquiries.
A: Predictive analytics identifies high-risk members, forecasts utilization, and anticipates fraud. Payers use it to:
- Stratify populations for care management.
- Forecast inpatient admissions.
- Detect suspicious billing patterns.
- Predict likelihood of appeal success.
A:
- GenAI → Personalized outreach, automated correspondence, and conversational agents for members.
- Agentic AI → Decision-making agents that can triage cases, trigger workflows, and handle prior auths end-to-end.
- Quantum AI (future trend) → Potential to optimize complex actuarial and risk-adjustment computations at scale.
A: We align outputs to business KPIs—cost per member per month, claims turnaround, Star ratings, and member satisfaction. Insights are delivered through dashboards, case manager workflows, and decision-support systems. Importantly, we quantify ROI from the pilot stage to win executive buy-in.
A: AI supports proactive interventions:
- Identify rising-risk members before hospitalization.
- Recommend next-best-actions to case managers.
- Personalize chronic disease outreach.
- Automate scheduling reminders and follow-ups.
A: AI directly influences HEDIS measures (screenings, adherence, chronic disease management). Closing these care gaps improves quality measures, which lift Star Ratings. Each 1-star improvement translates into significant CMS bonus revenue for Medicare Advantage plans.
A: Behavioral science enhances engagement. Instead of sending generic reminders, AI-tailored nudges—text, app push, call—are timed to maximize response. For example, one case study showed digital nudging increased care gap closure rates by double digits.
A: Claims leakage refers to revenue lost due to incorrect coding, fraud, or misprocessing. Typical leakage ranges from 3–7% of claims. AI-driven predictive audit models detect anomalies early, helping recover millions and reducing provider disputes.
A: By detecting patterns in billing, provider behavior, and member utilization. Techniques include anomaly detection, clustering, and supervised fraud classification. AI augments human auditors, enabling faster and more accurate fraud identification.
A: Yes. NLP + GenAI can read clinical notes, match them against policy rules, and approve routine requests instantly. This reduces manual workload, denial rates, and member/provider dissatisfaction. Agentic AI will further automate workflows end-to-end.
A: It forecasts high-cost procedures and admissions, helping payers design proactive interventions. For example, predicting likely readmissions enables early post-discharge outreach.
Q19. How critical is interoperability between payers and providers?
A: Extremely critical. Without it, providers submit incomplete claims, payers lack real-time clinical insights, and members fall through cracks. FHIR-based APIs, CMS mandates, and payer-provider data-sharing frameworks are breaking down these silos.
A: It’s a unified, longitudinal record of each member—integrating claims, EHR, pharmacy, labs, and social determinants. It fuels AI models, personalizes outreach, and enables a complete picture for care managers and actuaries.
A: Surveys by Bain show ~75% of payers are increasing IT spend, prioritizing cybersecurity, interoperability, AI, and care management platforms. CIOs are shifting from modernization to innovation and integration.
A: Competitors include EXL, Cognizant, Mu Sigma, and Optum’s analytics arms. Fractal GHIT Digital differentiates through Enterprise AI platforms, behavioral analytics expertise, and productized accelerators like Health Triage and Claims Anomaly frameworks.
A: Regulations like HIPAA and CMS Stars mean payers need explainable, auditable AI. Models must have transparent decision making, robust PHI protection, and audit logs. Regulatory risk is a major consideration in deployment.
A: AI can expose inequities in access or outcomes. By integrating SDOH data and testing for subgroup fairness, payers can design interventions for underserved populations, aligning with CMS and NCQA’s push for equity.
A: We’ll see:
- Widespread prior auth automation.
- Agentic AI-driven case management.
- GenAI chatbots replacing call centers.
- Advanced Member 360 platforms.
- Greater payer-provider data collaboration.
Ultimately, the focus will be on aligning cost efficiency with member experience and clinical quality.
Reach out to us for RFPs or ASK for DEMO
Monika Vashishtha, MBA, ITIL, PHP
646.734.6482