#GHITDigital #Providers #HospitalSystems #EHR #Interoperability #AI #GenAI #RCM #FHIR #ValueBasedCare
P2 (Providers) includes hospitals (academic, community), health systems, Independent Practice Associations (IPAs), ambulatory clinics, outpatient imaging and diagnostic centers, and specialty care networks. Providers deliver frontline clinical care across inpatient, outpatient, emergency, and virtual settings. Their technology backbone centers on EHR/EMR systems (Epic, Oracle/Cerner, Meditech, eClinicalWorks), but the clinical and operational ecosystem extends across imaging (PACS/VNA), labs (LIS/LIMS), medical devices (MRI/CT, monitors, infusion pumps), RTLS, RCM, ECM/archival platforms, and emerging AI/GenAI stacks.
This document follows a Q&A approach to present practical, technical, and strategic answers for CIOs, CMIOs, VPs of Clinical Operations, and technology delivery teams engaged in provider digital transformation.
A: P2 includes hospitals, health systems, IPAs, outpatient clinics, imaging/diagnostic centers and ambulatory networks. They operate clinical, operational and administrative systems — EHR/EMR at the core — plus imaging (PACS/VNA), labs (LIS/LIMS), RCM, device/IoT stacks, RTLS, supply chain and workforce systems.
A: Point-to-point HL7 v2 integrations, heterogeneous EHR estates after mergers, siloed imaging & archive systems, proprietary device interfaces, ungoverned data lakes, and outdated archival strategies (paper/scanned records).
A: Strategic integration (EHR connectors, FHIR façade), data governance, vendor consolidation roadmap, cloud and security strategy, cost-to-serve optimization, and enabling analytics/AI while minimizing clinician disruption.
A: Clinical safety, workflow fit, CDS rules, clinician adoption, AI validation/acceptance and ensuring that integration changes preserve care quality and reduce clinician cognitive load.
A: EHR connector pilots for acquisition harmonization, RTLS pilot for high-value assets (e.g., infusion pumps), imaging AI triage for ED CTs, and RCM automation for top-volume denial codes.
A: Clear KPIs (e.g., ED time-to-diagnosis reduction, denial rate drop), defined scope, clinician co-design, MLOps monitoring, and plans for scalability and governance.
A: Start with value mapping + shop-floor observations, co-design with clinicians, build a 90-day integration sprint (quick wins), and scale with low-code orchestration + MLOps. Emphasize pilot → measure → scale.
A: Involve clinicians from day one, iterate on UX with small changes, provide measurable time-savings, offer training, and run a continuous feedback loop embedded in the workflow.
A: Break into modular packages: Phase 0 discovery (fixed), Phase 1 integration backbone + quick wins (small-to-medium), Phase 2 pilots (medium), Phase 3 enterprise scale (large). Pricing mixes fixed-fee accelerators + time-and-materials for bespoke integrations.
A: Discovery (2–4 weeks), integration backbone + connectors (6–12 weeks), pilot for one workflow (8–12 weeks). Total from kick-off to pilot value: ~3–6 months depending on scope.
A: Core EHR/EMR (Epic, Cerner, Meditech, eClinicalWorks), PACS/VNA for imaging, LIS/LIMS for labs, RCM platforms, EHR connector/federation layer, FHIR façade/API gateway, device/MDI gateways, RTLS, ECM/archival (OpenText/NewgenOne), low-code BPM, cloud data lake and MLOps.
A: HL7 v2 (ADT, labs), DICOM (imaging), FHIR (APIs & modern apps), IHE profiles, and event-driven streams (Kafka) for device telemetry.
A: ED boarding, OR delays & late starts, low MRI/CT utilization, device downtime, high denial rates, data fragmentation across EHRs and inaccessible legacy data.
A: Deploy MDI gateways to normalize device telemetry, use predictive maintenance via IoT telemetry, and connect to CMMS for scheduled maintenance windows— all orchestrated via an integration plane.
A: Clinical note summarization, prior-auth and appeal drafting, discharge summary generation, patient communications, and clinician decision support augmentation — all requiring human review and governance.
A: Hallucinations, lack of provenance, PHI leakage risk, and clinician mistrust if outputs are inaccurate or opaque.
A: Model validation with clinical gold standards, bias & fairness testing, performance SLAs, versioning & rollback plans, clinician sign-off workflows, data lineage, and an AI ethics committee or steward.
A: De-identify data where possible, use private models or on-prem/cloud VPC boundaries, encrypt data in transit and at rest, and limit model access to authorized roles with audit trails.
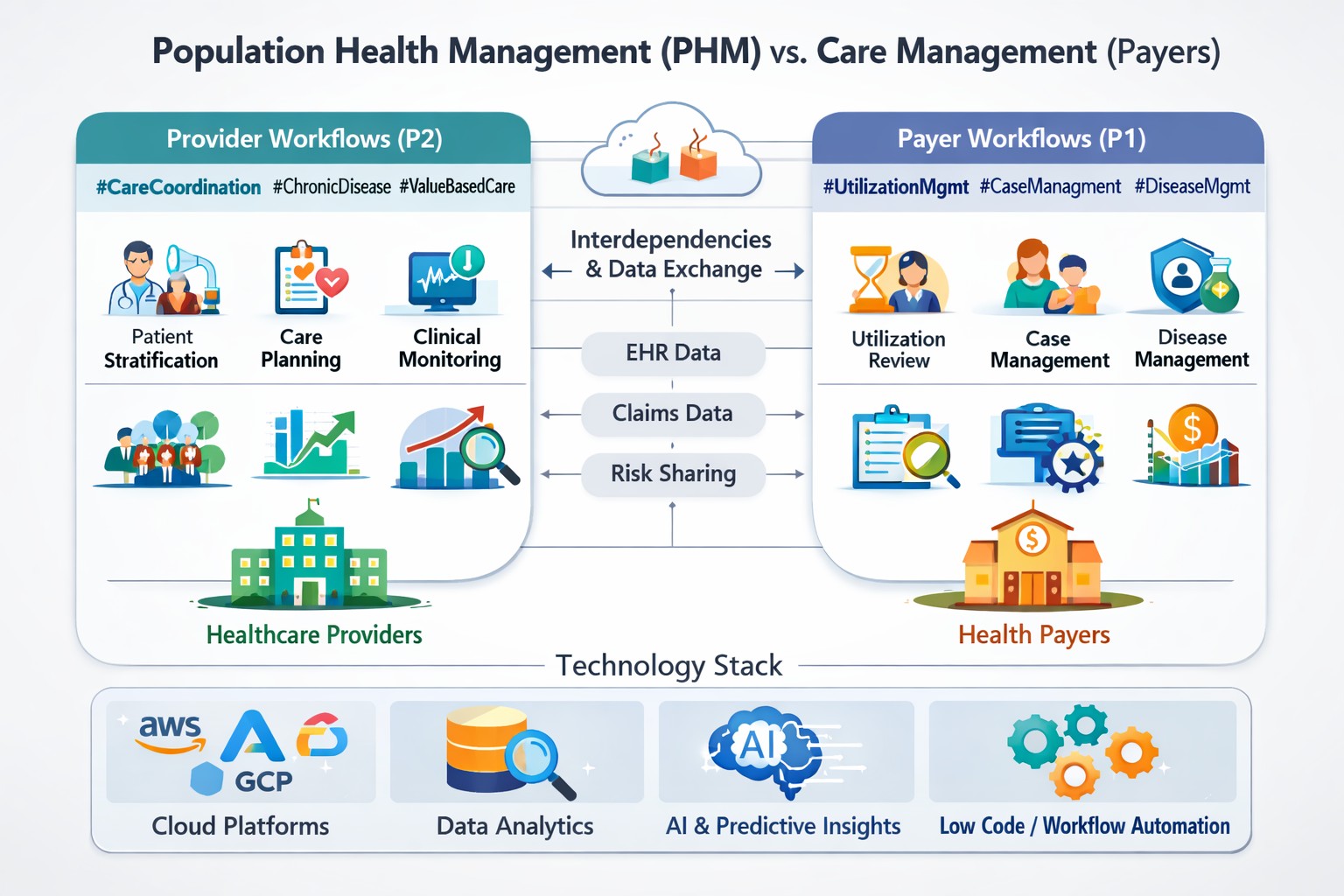
A: Providers need longitudinal data (claims + clinical), stronger care coordination, population health analytics, risk stratification, and aligned workflows with payers for shared savings.
A: Payers provide claims data, reimbursement models, prior-auth rules, quality measure definitions, and risk contracts. Providers rely on timely eligibility, authorizations and claims reconciliation — making payer integrations and data exchange critical.
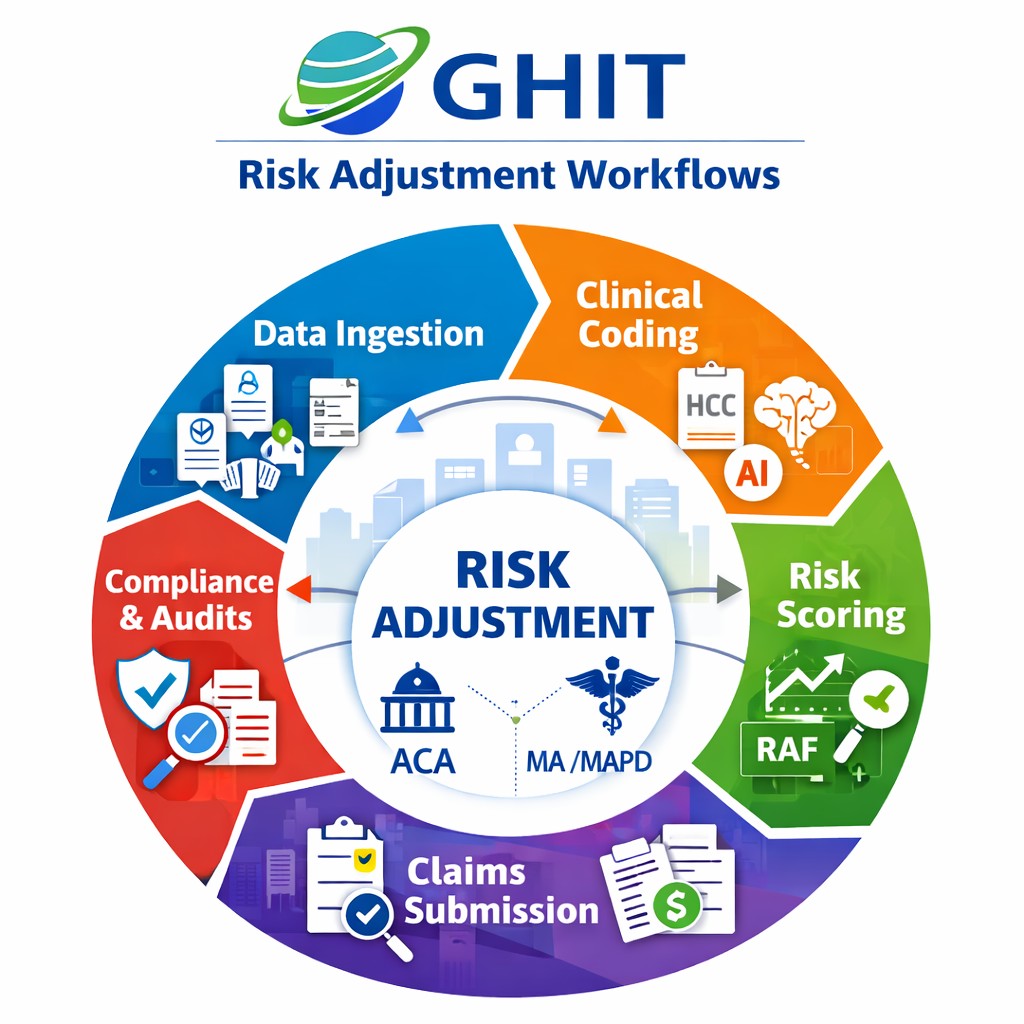
This supplemental section enumerates the end-to-end workflows that GHIT typically maps during discovery and implementation:
Representative vendors and partners GHIT frequently engages with:
Key metrics to measure success:
Governance & compliance must include HIPAA security controls, AI ethics & model validation, device security policies, and data retention/legal-hold procedures for archival systems.
GHIT can provide the following client-ready deliverables:
Providers must pursue a practical, phased interoperability and AI strategy: build a resilient integration fabric, use low-code orchestration to reduce time-to-value, operationalize AI with MLOps and clinician governance, and maintain robust archival strategies. GHIT Digital combines domain knowledge, pre-built accelerators and clinician co-design to deliver measurable outcomes across care, operations and revenue.
Contact GHIT Digital: contact@ghitdigital.com | +1 (856) 555-0100